Bioceramics exhibit excellent mechanical strength and chemical stability, making them ideal for load-bearing applications in bone implants, while bioactive glasses excel in promoting rapid bone regeneration due to their superior bioactivity and ability to form strong bonds with living tissues. The controlled degradation rates of bioactive glasses facilitate gradual replacement by natural bone, contrasting with the more inert nature of bioceramics, which tend to remain structurally intact over time. Advances in composite materials are combining the durability of bioceramics with the regenerative properties of bioactive glasses to enhance overall performance in orthopedic and dental applications.
Table of Comparison
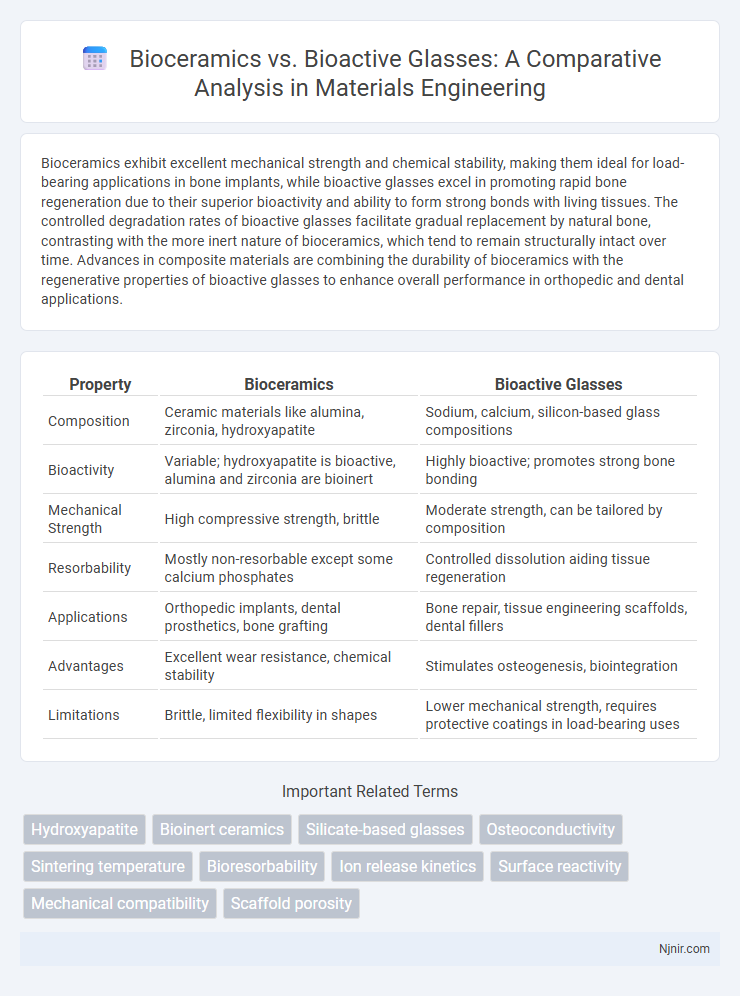
| Property | Bioceramics | Bioactive Glasses |
|---|---|---|
| Composition | Ceramic materials like alumina, zirconia, hydroxyapatite | Sodium, calcium, silicon-based glass compositions |
| Bioactivity | Variable; hydroxyapatite is bioactive, alumina and zirconia are bioinert | Highly bioactive; promotes strong bone bonding |
| Mechanical Strength | High compressive strength, brittle | Moderate strength, can be tailored by composition |
| Resorbability | Mostly non-resorbable except some calcium phosphates | Controlled dissolution aiding tissue regeneration |
| Applications | Orthopedic implants, dental prosthetics, bone grafting | Bone repair, tissue engineering scaffolds, dental fillers |
| Advantages | Excellent wear resistance, chemical stability | Stimulates osteogenesis, biointegration |
| Limitations | Brittle, limited flexibility in shapes | Lower mechanical strength, requires protective coatings in load-bearing uses |
Introduction to Bioceramics and Bioactive Glasses
Bioceramics are advanced ceramic materials specifically designed for medical applications, known for their high biocompatibility, bioinert or bioactive properties, and excellent mechanical strength, commonly used in bone grafts and dental implants. Bioactive glasses are a subclass of bioceramics composed primarily of silica-based glass systems that interact with biological tissues, promoting bone regeneration and bonding through the formation of hydroxycarbonate apatite layers. Their unique ability to stimulate cellular responses and support tissue repair distinguishes bioactive glasses from traditional bioceramics, making them critical in regenerative medicine.
Historical Development and Evolution
Bioceramics emerged in the 1960s, initially used for bone repair due to their chemical inertness and biocompatibility, with materials like alumina and zirconia gaining prominence. Bioactive glasses were developed later in the late 1960s, pioneered by Dr. Larry Hench, introducing materials capable of bonding with bone through surface reactions forming hydroxycarbonate apatite layers. The evolution of bioactive glasses expanded their medical applications beyond bone regeneration to include soft tissue repair, while bioceramics continued to evolve with improved mechanical properties and tailored bioactivity for diverse clinical uses.
Chemical Composition and Structure Comparison
Bioceramics primarily consist of calcium phosphates, such as hydroxyapatite and tricalcium phosphate, with a crystalline structure resembling natural bone minerals, promoting excellent biocompatibility and osseointegration. Bioactive glasses are composed mainly of silica (SiO2), sodium oxide (Na2O), calcium oxide (CaO), and phosphorus pentoxide (P2O5), featuring an amorphous, glassy structure that enables ionic exchange and formation of a hydroxycarbonate apatite layer on implantation. The differences in chemical composition and structural organization directly influence their bioactivity, degradation rates, and applications in bone regeneration and tissue engineering.
Mechanical Properties and Performance
Bioceramics exhibit high compressive strength and wear resistance, making them suitable for load-bearing orthopedic implants, whereas bioactive glasses offer lower mechanical strength but excel in bonding with bone through bioactivity and controlled degradation. The fracture toughness of bioceramics typically surpasses that of bioactive glasses, enhancing their durability under mechanical stress. Bioactive glasses compensate for their reduced mechanical performance by stimulating bone regeneration and integrating with surrounding tissues, improving overall implant success in non-load-bearing applications.
Bioactivity and Biological Interactions
Bioceramics exhibit excellent bioactivity characterized by their ability to form a direct bond with bone tissue through a stable hydroxyapatite layer, promoting osteoconductivity and biocompatibility. Bioactive glasses demonstrate superior bioactivity by releasing ionic dissolution products that stimulate cellular responses, enhancing osteogenesis and angiogenesis for improved biological interactions and tissue regeneration. Both materials possess distinct mechanisms of bioactivity, with bioactive glasses offering enhanced stimulation of molecular pathways critical for bone healing and remodeling.
Applications in Biomedical Implants
Bioceramics such as alumina and zirconia offer exceptional mechanical strength and wear resistance, making them ideal for load-bearing orthopedic implants like hip and knee replacements. Bioactive glasses, composed mainly of silicon dioxide, calcium oxide, and phosphorus pentoxide, excel in bone regeneration applications by bonding directly to bone and stimulating osteogenesis. The integration of bioactive glasses in dental and craniofacial implants enhances tissue repair and promotes faster healing compared to inert bioceramics.
Degradation and Resorption Behaviors
Bioceramics like calcium phosphates exhibit controlled degradation through ionic dissolution and cellular resorption, closely matching bone remodeling rates and maintaining structural integrity. Bioactive glasses degrade faster via surface ion exchange, forming a hydroxycarbonate apatite layer that promotes rapid tissue integration but with less mechanical stability over time. The distinct resorption behaviors influence their applications, where bioceramics suit long-term load-bearing implants and bioactive glasses excel in fast-regenerating bone defects.
Fabrication Techniques and Processing Methods
Bioceramics such as alumina and zirconia are commonly fabricated using powder processing techniques including sintering and hot isostatic pressing to achieve high mechanical strength and density. Bioactive glasses are typically produced through melting-quenching or sol-gel methods, providing molecular-level homogeneity and enhanced surface reactivity for bone bonding. Processing parameters for bioactive glasses are optimized to control porosity and bioactivity, while bioceramics emphasize crystallinity and mechanical integrity.
Challenges and Limitations
Bioceramics face challenges such as brittleness and limited toughness, which restrict their use in load-bearing applications, while bioactive glasses often exhibit poor mechanical strength and susceptibility to cracking under stress. Both materials must overcome issues related to long-term stability and biocompatibility, including potential degradation products that may elicit adverse biological responses. Optimizing these materials requires balancing bioactivity with mechanical integrity to ensure successful integration and functional longevity in biomedical implants.
Future Prospects and Emerging Trends
Bioceramics and bioactive glasses are advancing rapidly with emerging trends emphasizing enhanced bioactivity and tailored degradation rates for tissue engineering and regenerative medicine. Future prospects include the development of composite materials combining bioceramics and bioactive glasses to improve mechanical strength and biological performance in bone repair. Innovations in 3D printing and nanotechnology are driving personalized implant designs with increased osteointegration and controlled therapeutic ion release.
Hydroxyapatite
Hydroxyapatite, a key bioceramic, exhibits superior osteoconductivity and structural similarity to natural bone compared to bioactive glasses, making it highly effective for bone regeneration and implant integration.
Bioinert ceramics
Bioinert bioceramics, such as alumina and zirconia, offer exceptional mechanical strength and chemical stability but lack the bioactivity of bioactive glasses, limiting their ability to bond with bone tissue.
Silicate-based glasses
Silicate-based bioactive glasses exhibit superior bone bonding and controlled biodegradation compared to traditional bioceramics, making them highly effective for regenerative medicine applications.
Osteoconductivity
Bioceramics exhibit strong osteoconductivity by providing a stable scaffold for bone growth, while bioactive glasses enhance osteoconductivity through surface reactions that stimulate rapid bone bonding and regeneration.
Sintering temperature
Bioceramics typically require higher sintering temperatures above 1200degC, whereas bioactive glasses sinter at lower temperatures around 600-900degC, enabling better control of porosity and bioactivity.
Bioresorbability
Bioceramics generally exhibit limited bioresorbability, while bioactive glasses offer enhanced bioresorbability, promoting faster integration and gradual replacement by natural tissues.
Ion release kinetics
Bioceramics exhibit slower ion release kinetics compared to bioactive glasses, which rapidly release therapeutic ions to enhance bone regeneration and bioactivity.
Surface reactivity
Bioceramics exhibit limited surface reactivity primarily fostering mechanical stability, whereas bioactive glasses demonstrate high surface reactivity that promotes rapid formation of hydroxyapatite layers for enhanced bone bonding.
Mechanical compatibility
Bioceramics exhibit higher mechanical strength and wear resistance compared to bioactive glasses, which offer superior bioactivity but lower mechanical compatibility for load-bearing applications.
Scaffold porosity
Bioceramics typically offer controlled scaffold porosity for bone tissue engineering but bioactive glasses provide a more tunable and interconnected porous structure that enhances cell infiltration and vascularization.
Bioceramics vs Bioactive glasses Infographic